
From Dr. Joseph Mercola
Since COVID-19 first entered the scene, exchange of ideas has basically been outlawed. By sharing my views and those from various experts throughout the pandemic on COVID treatments and the experimental COVID jabs, I became a main target of the White House, the political establishment and the global cabal.
Propaganda and pervasive censorship have been deployed to seize control over every part of your life, including your health, finances and food supply. The major media are key players and have been instrumental in creating and fueling fear.
I am republishing this article in its original form so that you can see how the progression unfolded.
Originally published: July 19, 2020
Denis Rancourt, Ph.D., a former full professor of physics, is a researcher with the Ontario Civil Liberties Association in Canada. He’s held that volunteer position since 2014, which has given him the opportunity to dig into scientific issues that impact civil rights. He also did postdoctoral work in chemistry.
Here, we discuss the controversial topic of face masks. Should you wear one? When and where? Does it protect you or not? There’s a wide range of opinions on this even within the natural health community.
Early on in the COVID-19 pandemic, I endorsed the use of face masks based on the experience of some of the Eastern European countries. The rationale of it seemed to make sense at the time. Since then, however, I’ve started to question their use.
Unfortunately, the mainstream propaganda and government orders in many states reverted back toward mask wearing just about everywhere. You’re not allowed into stores; you cannot fly or take a cab, Uber or Lyft without one; you must wear one everywhere you go, even outdoors, and if you don’t you’re vilified, sometimes aggressively attacked.
There’s No Scientific Support for Mask-Wearing
Rancourt’s investigation into mask wearing was part of his research for the Ontario Civil Liberties Association. He did a thorough study of the scientific literature on masks, concentrating on evidence showing masks can reduce infection risk, especially viral respiratory diseases.
“What I found when I looked at all the randomized controlled trials with verified outcome, meaning you actually measure whether or not the person was infected … NONE of these well-designed studies that are intended to remove observational bias … found there was a statistically significant advantage of wearing a mask versus not wearing a mask.
Likewise, there was no detectable difference between respirators and surgical masks. That to me was a clear sign that the science was telling us they could not detect a positive utility of masks in this application.
We’re talking many really [high-]quality trials. What this means — and this is very important — is that if there was any significant advantage to wearing a mask to reduce this [infection] risk, then you would have detected that in at least one of these trials, [yet] there’s no sign of it.
That to me is a firm scientific conclusion: There is no evidence that masks are of any utility either preventing the aerosol particles from coming out or from going in. You’re not helping the people around you by wearing a mask, and you’re not helping yourself preventing the disease by wearing a mask.
This science is unambiguous in that such a positive effect cannot be detected. So, that was the first thing I publicized. I wrote a large review1,2 of the scientific literature about that.
But then I asked myself, as a physicist and as a scientist, why would that be? Why would masks not work at all? And so, I looked into the biology and physics of how these diseases are transmitted.”
The Importance of All-Cause Mortality Statistics
When trying to tease out whether an intervention works against COVID-19 or not, it’s important to look at death statistics. The number of deaths is really what’s important, not the number of infected individuals, as many may not even exhibit symptoms.
The problem is that assigning the cause of death in a situation where a viral infection taxes the immune system and is confounded by comorbidities is tricky business. As noted by Rancourt, epidemiologists have long known that you cannot reliably assign cause of death during a viral pandemic such as this. There’s tremendous bias involved.
To get around those problems, you have to look at all-cause mortality. The reason for this is because all-cause mortality data are not affected by reporting bias.
So, Rancourt did a detailed study of the current data of all-cause mortality, showing that the all-cause mortality this past winter was no different, statistically, from previous decades. In other words, COVID-19 is not a killer disease, and this pandemic has not brought anything out of the ordinary in terms of death toll.
Government Lockdown Orders Fueled Death Toll
He published this data in the paper,3 “All-Cause Mortality During COVID-19: No Plague and a Likely Signature of Mass Homicide by Government Response.” Rancourt explains:
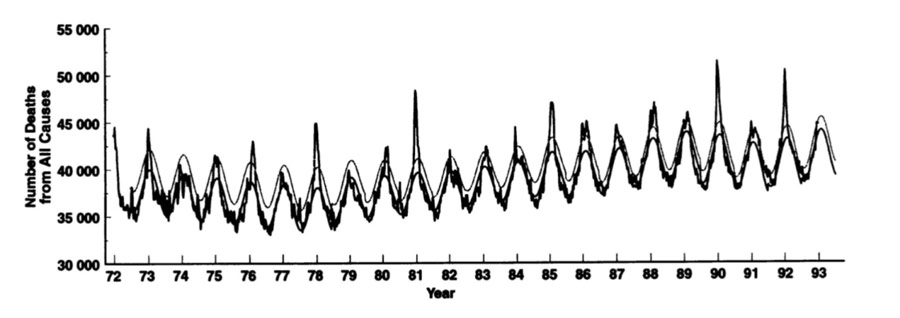
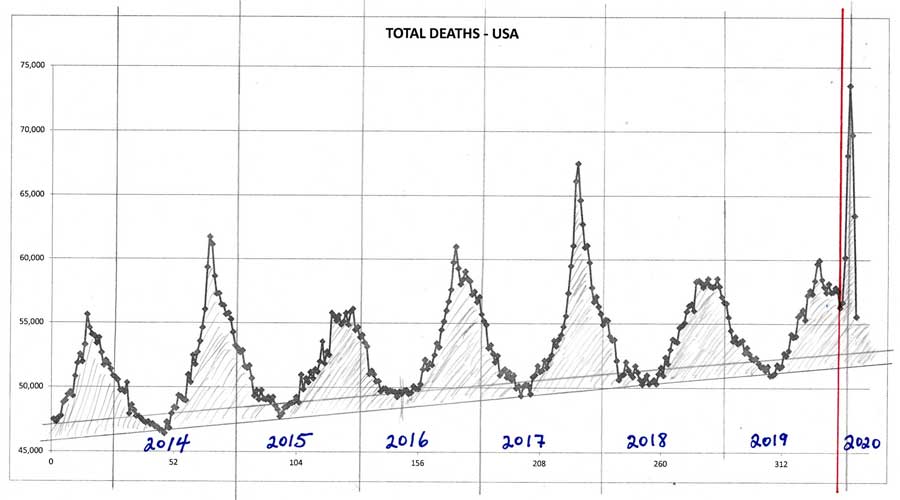
“It turns out that these curves, which show the winter burden deaths as humps every winter, some of them, in some jurisdictions, have an additional very sharp peak. It doesn’t represent a … huge amount of deaths by comparison to the total winter burden because it’s a very sharp peak, but it’s an anomalous peak. It’s not a natural peak.
And it happened in exact coincidence and time everywhere. In every jurisdiction that sees this anomalous, unnatural peak … the peak started exactly when the pandemic was declared by the World Health Organization. And the World Health Organization at that time recommended states prepare their hospitals for a huge influx of people with critical conditions.
So, the government response to that World Health Organization recommendation is what killed people, what accelerated the deaths. You can see that in the data, and you can also understand it in terms of how immune-vulnerable people are affected by these kinds of diseases.
What they did is they closed people into their institutional places of residence, they didn’t allow visitors. So, they isolated the most vulnerable parts of society that already had comorbidity conditions who were in a fragile state.
So, they ensured that many people that were locked into these institutions would die from this particular seasonal virus that causes the respiratory disease.
But the virus itself is not more virulent than other viruses. The total winter burden deaths is not greater, but there is a signature of a sharp feature that lasts the full width at half maximum. This feature is three or four or five weeks, which is extraordinarily rapid, never been seen before. And it happens very late in the winter burdens season.
A sharp peak like this has never been seen this late in the season before, and it’s happening [synchronistically] everywhere, on every continent, at the same time in direct immediacy after the declaration of the pandemic. To my eye, there is no doubt that there was an acceleration of deaths of vulnerable people due to government responses …
What really matters is the hard data, and the hard data is all-cause mortality in any jurisdiction that you want to look at. And it has not been anomalous, statistically speaking, no matter how you slice it.”
The two graphs below show the number of deaths from all causes from 1972 until 1993, and 2014 until present time in 2020.
Why Government Response Was Ill Advised
Rancourt goes on to qualify some of this data based on the mechanism of viral transmission, which also helps explain why government responses have been ill advised, as they actually worsen transmission rather than inhibit it. Infectious respiratory diseases primarily spread via very fine aerosol particles that are in suspension in the air.
“We’re talking about the small size fraction of aerosols, so typically smaller than 2 micrometers,” Rancourt explains. “There are water droplets that bear these virions, the virus particles, and there can be dozens or hundreds of these virions per very small droplet of this size.
Those are the droplets we’re talking about. When you get down to those sizes, gravitational outtake is very inefficient and they basically stay in suspension. And, as soon as you have currents or flow of air, [the particles] are carried.”
The aerosol particles stay in suspension when the absolute humidity is low. This is why influenza outbreaks occur during the winter. Once absolute humidity rises, the aerosol particles become unstable. They agglomerate, drop out of suspension and cease to be transmissible. “This is well known,” Rancourt says. “It’s been known for a decade. It’s been extraordinarily well-demonstrated by top scientists.”
The mid-latitude band is where you find the dry weather and the temperature ideal for transmitting viral respiratory diseases. Viral infections typically spread during the winter in the northern hemisphere, and in the summer in the southern hemisphere.
“You see it in both hemispheres, but inverted,” Rancourt says. “That is why, when you move down towards the equator, transmission drops. You don’t get transmission.
Likewise, if you go too far North, it also does not transmit, and that is not well understood. I’m an expert in environmental nanoparticles and how they charge and what they do, so I have some ideas about why that is, but it hasn’t been studied in detail.
The point is the transmission band is very narrow. It’s across Europe and North America where you have temperatures between about zero and 10 degrees Celsius, and you have low absolute humidity. That’s where these aerosol particles that are the vector of transmission are completely suspended as part of the fluid air.
They’re really part of the fluid air, so any air that gets through, [the viral particles are also] going to come through. That’s why masks don’t work. And these particles are in suspension in the air and get trapped indoors.
That’s why centers where you have sick people and you’re not controlling the air environment are centers of transmission. We’re talking about old folks’ homes, hospitals, even people’s homes. This entire class of diseases, this is how they’re transmitted.”
Why Masks Are Used During Surgery
Many firmly believe wearing a mask in public will protect themselves and/or others, and one of the reasons for this is because they appear to work in some circumstances, such as operating rooms. If they don’t work, why do surgical staff and many health care workers use them on a regular basis?
As explained by Rancourt, the reason surgical masks are worn in the operating room is to prevent spittle from accidentally falling into an open wound, which could lead to infection. Surgical masks have been shown to be important in that respect.
Preventing microbes and bacteria from falling into an open wound is very different from preventing the spread of viral particles, however. Not only are viruses much smaller than bacteria and many other microbes found in saliva, they are, again, airborne. They’re aerosolized and part of the fluid air. Therefore, if air can penetrate the mask, these aerosol particles can also get through.
“The best randomized controlled trials with verified outcome — in other words, the only scientifically designed studies that remove observational bias and that are valid and rigorous — are [done] in clinical environments.
So, they’re looking at health care workers treating people that potentially have a viral respiratory infection, or treating people they know have such an infection and they’re doing something that will potentially generate a lot of aerosol particles by the treatment. Many, many trials have been done in that environment and none of them find any advantage to the health care workers,” Rancourt says.
Mask Wearing Does Not Protect Others Either
The video below is from Patrick Bet David, who has a very popular YouTube channel that I enjoy watching. His message below is broken down into very simple terms and he presents valid arguments and good questions. I encourage you to view it if you believe in wearing masks.
Now, one view is that, even though a mask may not protect the wearer against contracting an infection, it will still protect others that the mask-wearer comes into contact with. But that’s not what the science shows. The measured outcome in most rigorous studies on this is the infection rate. Did anyone involved get infected?
Comparisons are made between health care workers wearing masks, respirators or nothing at all. While this does not allow you to discern who is being protected — the mask wearer or others — the studies show mask wearing does neither.
Since everyone is in close proximity to each other, and no differences in infection rates are found regardless of what type of mask is worn, or none at all, it tells us that mask wearing protects no one from viral infections.
“It makes no difference if everybody in your team is wearing a mask; it makes no difference if one is and others aren’t,” Rancourt says. “Wearing a mask or being in an environment where masks are being worn or not worn, there’s no difference in terms of your risk of being infected by the viral respiratory disease.
There’s no reduction, period. There are no exceptions. All the studies that have been tabulated, looked at, published, I was not able to find any exceptions, if you constrain yourself to verified outcomes.”
What’s more, the results are the same for both N95 respirators and surgical masks. Respirators offer no protective advantage when it comes to viral infections.
“In one of the randomized control trials, a big one that compared masks and N95 respirators among health care workers, the only statistically significant outcome they discovered and reported on was that the health care workers who wore the N95 respirators were much more likely to suffer from headaches,” Rancourt says.
“Now, if you’ve got a bunch of health care workers, which you’re forcing to get headaches, how good is the healthcare going to be?”
Why Masks Don’t Prevent Viral Infections
As noted by Rancourt, it’s important to separate scientific findings from possible mechanics that might explain a certain outcome. Studies have conclusively proven masks do not prevent viral infections. Why, is another question.
“I think it’s important to recognize that no matter how clever your explanation is, it may not be right,” he says. That said, one commonsense explanation put forth by Rancourt is that masks don’t work for this application for the simple fact that they allow airflow:
“I’ve come to the conclusion that the most prominent vector of transmission is these fine aerosol particles. Those fine aerosol particles will follow the fluid air. In a surgical mask, there is no way you’re blocking the fluid air. When you breathe wearing a surgical mask, the lowest impedance of airflow is through the sides and tops and bottoms of the mask.
In other words, very little of the airflow is going to be through the actual mask. The mask is only designed and intended to stop your spitballs from coming out and hitting someone … If the flow of air is through the sides, whatever molecules or small particles are carried in the air, are going to flow that way as well, and that’s how you get infected.
If you’re not stopping [the viral particles] coming in, you’re not stopping them from coming out either. They follow the flow, period. That’s the way it is. So that’s why there’s an equivalence between ‘It doesn’t protect you and it doesn’t protect anyone else either.’”
Ironically, some masks are even designed with out-vents, to facilitate breathing, which completely negate the claim that mask-wearers are protecting others.
Why Masks Have No Impact on Viral Load
Rancourt also dismisses the argument that masks can reduce the total viral load by catching your spit. The theory is that by minimizing the viral load someone is exposed to, their chances of the infection taking hold are minimized.
“The large droplets drop to the floor immediately and are not breathed in. So, they’re not part of the transmission mechanism. You can do a scientific study that demonstrates that viruses survive a fairly long time on a surface … These are called fomites, these surfaces where viruses can live and stay active.
That does not mean that transmission occurs through surfaces. It only means that a scientist was able to establish that a virus can survive a long time on a surface. It doesn’t tell you anything about the likely transmission mechanism of the disease. So, there are a lot of studies like this that are basically irrelevant in terms of transmission mechanism.
[Infectious respiratory diseases] are transmitted by these fine aerosol particles that are in suspension in the air. In a case like that, will a mask, will something that is preventing spitballs from coming out, protect you or protect others? And the answer is no, it makes no measurable difference.
There are many studies that show how difficult it is to actually infect someone when you’re just trying to put something like a fluid or something you know is bearing the virus into their eye or into their nose. It’s hard to do this. That’s what the studies show.
But if you take a fine aerosol and you breathe it in deeply, that’s where the infection starts and that’s where the virus has evolved to be most effective. So, by breathing in aerosols laden with these viruses, you’re going to be infected. Try to do anything else, and it’s going to be difficult [to spread infection].
The most recent randomized controlled trial [published] this year basically concluded they could find no evidence that masks, hand-washing and distancing, in terms of reducing the risk of these types of diseases, were of any use. [They] didn’t help.
So, there’s this dissonance between what the science actually tells you when you measure correctly, and what the health authorities tell you to do. They want you to be convinced that you’re in this dangerous environment and that if you follow their directives, you’ll be safe.
Their purpose is to control your life and to give you directives, and you’re going to accept that. That’s part of how they convince you that you absolutely need the state to save your life. I think that’s what’s going on.”
Mask-Wearing Is Not Without Its Risks
We’ve already mentioned that certain masks can increase your likelihood of headaches. Others believe masks can cause lower partial pressure of oxygen, which could cause serious health problems. In the video above, Peggy Hall with TheHealthyAmerican.org claims certain masks can result in low oxygen levels, thus violating OSHA rules on oxygen requirements.
“There are many admitted dangers to wearing masks,” Rancourt says. “The World Health Organization in its June 5 memo,4 where they reversed their position and decided that it was a good idea to recommend mask use in the general population, in that document, they actually say you have to consider the potential harms, and they list what they consider are all the potential harms.
They missed a lot. But one of the top ones is you’re concentrating the pathogen laden material onto this material near your face, nose, eyes and so on. And you’re touching the mask all the time, you’re touching yourself, you’re touching others.
It’s not a controlled clinical environment, so there’s potential for transmission in that way. You might wear the mask more than once, you might store it at home and then wear it again. You might do all kinds of things …
What I find extraordinary is that they also have a list of what they call potential advantages. And when I compare the two lists, the potential dangers far outweigh the potential advantages. So, you have to ask yourself, what the heck are you doing?
How can you make these two columns and compare the advantages and disadvantages and have one clearly outweigh the other and then conclude that therefore we recommend masks? This is just nonsense. It’s irrational. So, my association added our list5 of things that they weren’t even considering.
We went into the civil liberties aspect of it as well, because I think this is very important. One of the fundamental aspects of a free and democratic society is that the individual is entitled to evaluate the personal risk to themselves when they act in the world.”
As noted by Rancourt, risk evaluation is a very personal thing. It involves your personality, your judgment, your knowledge, your experience and your culture. It’s a very personal thing that you’re entitled to do for yourself. If the state is forcing you to accept their evaluation of risk, then this fundamental precept is violated. What’s worse, they’re forcing you to accept an evaluation of risk that cannot be scientifically justified.
Mask Mandates Are Indicative of Rising Totalitarianism
In its letter6 to the WHO, the Ontario Civil Liberties Association also addressed the issue of mask mandates as an instrument of totalitarianism.
“In our letter, we put it this way. There’s a recent scientific study7 that came out in 2019. The first author is the executive director of the Ontario Civil Liberties Association that I do research for, and he’s a physicist also. He wrote an article with another physicist.
They looked at the conditions under which a society will gradually degrade towards a more totalitarian state. What they found was that there were two major control parameters that characterize the society that will tell you if that is likely to happen or not.
One of those control parameters is authoritarianism in the society. What they mean by that is, how successful can an individual be to refuse something, like to refuse to wear a mask if they protest? What is the chance that they’ll succeed if they refuse? That would be related to the degree of authoritarianism.
The other important parameter is the degree of violence in the society. How violent is the repression if you disobey? So how big is the fine? Can you go to jail? How much punishment will you be subjected to if you disobey a particular rule, for example, wearing of a mask?
Those two parameters, they were able to establish what we call a phase diagram of societies … And what they found is that in present society, if you would estimate the average value of those two parameters for United States or Canada, we’re in a state right now where the society is very gradually evolving towards totalitarianism.
The way to slow that and prevent it is for people to object and to scale it back. As soon as you agree with an irrational order, an irrational command that is not science-based, then you are doing nothing to bring back society towards the free and democratic society that we should have. You are allowing this slow march towards totalitarianism. That’s how I would explain the importance of objecting to this.”
Mask Mandates Allow Government to Shirk Responsibility
Rancourt also points out that when government and health institutions convince people that masks are the solution, they are effectively removing their duty of care toward you, because they’re saying all you need to do is wear a mask. This allows them to avoid the responsibility of actually preventing transmission in the primary centers of transmission, such as hospitals, nursing homes and elsewhere.8
“We don’t have to manage the air in such a way that immune-vulnerable in this establishment will not be at risk of dying and so on. They remove their duty of care responsibilities by saying, ‘Well, we’re just not going to allow visitors, and we’re going to force everyone to wear masks.’
You need to look at, scientifically, what is happening here. Why are people at risk? What is immune-vulnerability due to? What can you do about it? And then you have to do something about it if you’re serious about your duty of care towards these people. So it has that side effect of letting them get away with not taking care of the people that they’re responsible for.”
Calls for Peaceful Civil Disobedience Are Growing
The Ontario Civil Liberties Association has issued a press release9 calling for peaceful civil disobedience against mandatory masking. The U.S. nonprofit Stand for Health Freedom is also calling for civil disobedience, and has a widget you can use to contact your government representatives to let them know wearing a mask must be a personal choice.
“In the memo that was put out, we explain how best to perform that civil disobedience. We explain that you should be calm and confident and not get into arguments and not try to convince the authorities.
Just express your disobedience regarding this rule. And then we explain that they may want to trespass you, they may want to give you a fine, that you can anticipate fighting that fine in court. We go through the steps so that people can visualize how to do this.
We explain that some of their core shoppers or core citizens will be angry and aggressive, and to not get into a fight and not to get into a war of words. Do not try to convince them. Just stick to that you are not going to comply. Be very calm. This kind of civil disobedience has been successful at various times in North American history.
There are risks involved, but it’s often worth it to the individual to have that civil disobedience because there are many individuals that don’t know what to do that are very angry because they’re being forced to wear masks and they see it as absurd and a constraint. So, we try to give them a view of a venue on how to resist this …
We also recommend when people are practicing this kind of civil disobedience that they not be isolated, that they try to form a grassroots group of support and that they don’t do it alone. Try to bring at least one person, one supporter, with them. Record the interaction with the authorities and report back on social media and to their groups with details of what happened and so on.
We hope to create kind of a smoother messaging that a lot of people, or at least some people, do not believe this mask story and do not believe that they are at risk and are willing to practice civil disobedience to make that point.”
